

Fox6Now.com: Tomah VA dentist accused of using improperly cleaned tools resigns
I shouldn’t read news as I always have something to say about them. This news above reminded me about working in the UK and how the instruments were cleaned there.
This Thomas VA dentist is not the only dentist that is underperforming in the instrument cleaning. There are dentists who have read this news and have wiped sweat from their foreheads and thanked their lucky stars it wasn’t their name on the headlines. Honestly!
Let me tell you how things were done in six of the practices I used to work in the UK. I will first go through the correct way of cleaning the instruments.
This I How It Should Be Done
1. Disinfect the contaminated instruments preferably in a washer disinfector like Miele Dental Disinfector
With this washer disinfector the cleaning job is half done. You just put used instruments within 4 hours of using them to the washing cycle and you get disinfected instruments in less than an hour (no need to soak them in anything prior the cycle).
No scrubbing is needed which will minimise the accidents of nurses cutting themselves.
2. Dry the instruments thoroughly. Use pressurised air on all the hard-to-reach areas like matrix retainers, sonic scaler tips, forceps.
3. Place the instruments that don’t need to be sterile on the metallic tray to be autoclaved. Put the instruments that need to be sterile in pouches and close the pouches.
4. Put all the instruments in an up-to-date vacuum autoclave and run the cycle. Once they are cooked, put them in cupboards or drawers to be picked to the surgeries.
Simple and pathogen-free tools.
This Is How It Should Not Be Done
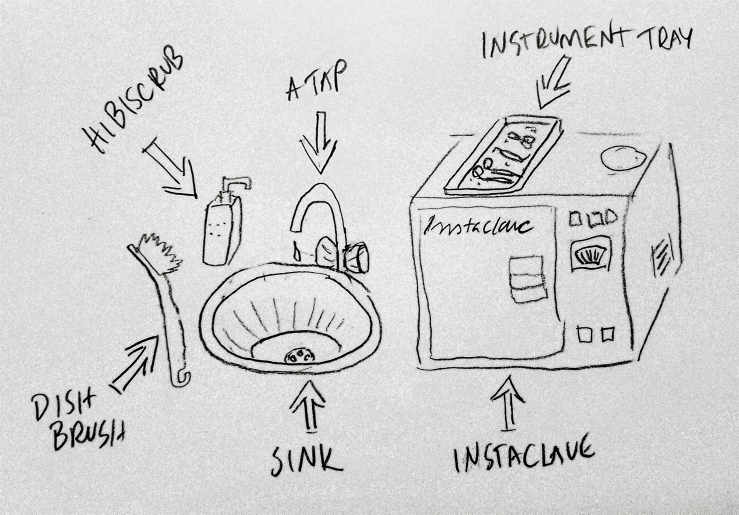
None of the surgeries I worked at in the UK had washer disinfector. Instead there was a dish brush and Hibiscrub. Yes, you read it correctly. Hibiscrub was used like washing up liquid on dish brush and the instruments were washed over a sink in the surgery. But this was done only up until health and safety regulations stated that using dish brush was a health hazard – there was too big risk of an injury from sharp instruments.
Once the instruments were brushed with Hibiscrub and rinsed with water, the instruments were placed on metallic trays (no drying) and put in the Instaclave, the simplest of the simplest model (non-vacuum). If there were surgical instruments, they were either put on the pouches and put on trays without closing the pouch. The pouch was closed after the cycle in the Instaclave. Sometimes the surgical instruments were put on the trays without pouches and once they had gone through the cycle, the nurse put them in the pouches that were taken straight from the package. This of course meant that the pouch was non-sterile as it had not gone through the cycle in the autoclave. Non-sterile pouch equals non-sterile instrument – no matter if the instrument has gone through the cycle.
So needless to say that many things went wrong. And let me clarify that all the above was done in the surgery. Every surgery had their own autoclave – just about five feet away from the patient.
The Question: Did I Do It Too?
Well, as much as I think that you live by the rules of the country you are in, I did not follow this questionable way of cleaning instruments. I did inventory on surgery’s storage room and found a container with a lid. I asked the practice manager to order me instrument disinfection liquid. I had to do some convincing before the liquid was ordered – understandably of course as no-one else was using one. So why should I?
So all my instruments were brushed with dish brush under running water and then placed into this container which had disinfection liquid in it. The instruments were kept in there for the recommended time, rinsed with water, dried and then put in the Instaclave.
Not perfect, but enough for me to have a clean conscience.
If you liked this post, you might also like:


